Anticipating and recognizing respiratory decompensation is only the first step in emergency airway management. Practitioners must be familiar with the indications and techniques for airway intervention and how to anticipate a difficult airway. The basic approach includes assuring airway patency, protection from aspiration, and providing adequate oxygenation and ventilation. This image shows the use of a GlideScope® (Verathon Inc.; Bothell, Washington) video laryngoscope to intubate the trachea of a morbidly obese patient with challenging airway anatomy. Image courtesy of Wikimedia Commons

Upper airway patency can be determined by assessing for stridor, drooling, hoarseness, edema, and facial trauma or burns. The most common cause of airway obstruction in the supine patient with a reduced level of consciousness is the tongue (yellow arrow). The head-tilt chin-lift maneuver gently extending the head slightly into the "sniffing position" (right image) and lifting the tongue from the back of the throat is the most reliable method of opening the airway when cervical spine injury is not suspected. Hyperextension of the neck is not recommended and may actually cause obstruction. Images courtesy of Wikimedia Commons

Airway adjuncts relieve upper airway obstruction caused by the tongue by lifting the tongue from the back of the hypopharynx. Airway adjuncts provide a conduit for ventilation, oxygenation, and suctioning and can be used with bag-valve-mask (BVM) ventilation. The oropharyngeal airway (OPA; left image) comes in a variety of adult and pediatric sizes and is sized from the corner of the mouth to the earlobe (right image). With a tongue blade to depress the tongue, the OPA is inserted over the tongue. Alternatively, the OPA can be placed upside down into the patient's mouth with the tip aimed at the soft palate and rotated 180°. OPAs are contraindicated in patients with a gag reflex because they may cause vomiting and aspiration and are poorly tolerated

Another airway adjunct is the nasopharyngeal airway (NPA). NPAs, like the OPA, can help prevent upper airway obstruction caused by the tongue. However, the NPA can be used in a conscious patient with an intact gag reflex. NPA devices can be inserted bilaterally if necessary. NPAs are measured from the nostril to the earlobe and are inserted with the bevel toward the nasal septum straight back along the floor of the nose (shown) until the flare rests against the nostril. Use of water-based surgical lubricant and choosing the larger of the 2 nostrils can make insertion less traumatic. Due to the risk for epistaxis or nasopharyngeal injury, NPAs are contraindicated in patients who are anticoagulated; have basilar skull fractures, nasal deformities, or nasal infections; and pediatric patients

BVM ventilation is the most important skill in basic airway management. Simple maneuvers and basic airway adjuncts can ensure a patent airway and allow for effective oxygenation and ventilation until a more definitive airway is established. BVM ventilation requires a good mask seal and a patent airway. The presence of facial hair, absence of teeth, obesity, and anatomic irregularities are factors that can make BVM ventilation difficult. Masks come in many sizes including newborn, infant, child, and adult. Choosing the appropriate size will help to create a good seal and effective ventilation

While providing BVM ventilation, extend the patient's head slightly using the head-tilt chin-lift maneuver. If cervical spine injury is suspected the modified jaw-thrust technique is used instead. Place an OPA or NPA to assist with ventilations. The mask should cover the nose and mouth without extending over the chin. The mask is held in place with the 1-handed E-C technique. Using the nondominant hand, create a C shape with the thumb and index finger (left image) over the top of the mask and apply gentle downward pressure. Hook the remaining fingers around the mandible taking care not to apply pressure to the soft tissues of the neck, and lift it upward toward the mask creating the E (right image). Leave dentures in place to improve mask seal

The 2-handed technique is preferred if a second person is available to provide ventilations. Create 2 opposing semicircles with the thumb and index finger of each hand to form a ring around the mask connector, and hold the mask on the patient's face. Lift the mandible with the remaining digits (left image). Alternatively, place both thumbs opposing the mask connector and use the thenar eminence to hold the mask to the face while lifting the mandible with the fingers (right image)

Endotracheal intubation is a critical, often lifesaving procedure for severely ill or injured patients who cannot maintain adequate oxygenation, perform effective ventilation, or maintain a protected airway. Intubation is also often used when a patient is at risk for serious deterioration or is considered unstable and needs a procedure or transfer that requires leaving the resuscitation room environment. Intubation is usually performed with a conventional laryngoscope (shown), flexible fiberoptic bronchoscope, or video laryngoscope. Proper airway management requires a thorough understanding of the indications for tracheal intubation, the pharmacology of sedative and neuromuscular-blocking agents used in rapid sequence intubation (RSI), and the proper methods for endotracheal tube placement

Prepare your equipment: Endotracheal tubes (ETT) (shown) come in a number of sizes, usually designated in millimeters of internal diameter. The choice of ETT size is always a compromise between choosing the largest size to maximize flow and minimize airway resistance and the smallest size to minimize airway trauma. A high-pressure/low-volume balloon at the distal tip is inflated after insertion and effectively seals off the trachea preventing aspiration and ensuring adequate ventilation and oxygenation. A malleable stylet should be used during intubation to provide shape and strength to the ETT. It is inserted into the lumen of the ETT with the tip 1-2 cm from the distal end of the ETT. Do not let the stylet protrude beyond the ETT tip because this may cause airway trauma. Image courtesy of Wikimedia Commons

The laryngoscope is a rigid instrument used to facilitate intubation of the trachea. The 2 main components are a cylindrical handle (left) and the blade. The most commonly used blades in the United States are the Macintosh and the Miller. The curved Macintosh (center) is designed to have the tip placed in the vallecular space anterior to the epiglottis. The epiglottis is then elevated indirectly to expose the vocal cords. The Miller blade, which is straight, is placed under the epiglottis, which is lifted directly to expose the vocal cords (right). Both blades come in a variety of sizes. The choice of blade depends on personal preference and patient anatomy

Setting up and preparing for intubation includes checking that all equipment is working. Oxygen with face mask or BVM is available or currently being used to preoxygenate the patient. Suction is available, working and within hands reach. You should always anticipate a difficult airway and have rescue airway equipment such as a coude-tip bougie (shown), laryngeal mask airway (LMA), GlideScope, or surgical cricothyrotomy kit available

When pre-oxygenating using manual ventilations with the BVM (shown), remember to squeeze the bag once every 5 seconds delivering volumes just enough to cause the chest to rise. Gastric inflation can occur when the bag is squeezed too forcefully or too quickly. The ventilatory rate should not exceed 10-12 breaths per minute. Use a tidal volume of approximately 8-10 mL/kg or just large enough to cause chest rise. During cardiopulmonary resuscitation, smaller tidal volumes (5-6 mL/kg) are adequate because of the reduced cardiac output of such patients. Contraindications to bag-valve mask include severe facial trauma and airway obstruction. A surgical airway is often indicated in these patients

A difficult airway assessment must be performed before attempting intubation, especially when using neuromuscular-blocking agents. The mnemonic "LEMON" is a helpful tool to focus on evaluation for a potentially difficult airway. "L" = Look for signs of obesity, micrognathia, evidence of previous head and neck surgery or irradiation, facial hair, poor dentition, dentures, large teeth, a narrow face, a high and arched palate, a short or thick neck, and facial or neck trauma. "E" = Evaluate the 3-3-2 rule. Normal mouth opening is 3 of the patient's fingerbreadths. Hyomental distance (left image) when measured should be at least 3 fingerbreadths, whereas the thyrohyoid distance (right image) should be at least 2 fingerbreadths

"M" is for Mallampati classification, which is performed with the patient seated and neck extended. Open the patient's mouth fully; protrude the patient's tongue; and say "ah." The classes are as follows: Class I: soft palate, uvula, fauces, and pillars visible = no difficulty; Class II: soft palate, uvula, and fauces visible = no difficulty; Class III: soft palate and base of uvula visible = moderate difficulty; Class IV: only the hard palate is visible = severe difficulty. Image courtesy of Wikimedia Commons
"O" is for Obstruction. Evaluation for foreign bodies (arrow), stridor, and other forms of sub- and supraglottic obstruction should be performed in every patient prior to laryngoscopy.
"N" is for Neck mobility. Patients with degenerative or rheumatoid arthritis may have limited neck motion, and this should be assessed to ensure the ability to adequately extend the neck during laryngoscopy and intubation. Patients in whom traumatic cervical spine injury (shown) is suspected and in whom the cervical spine has been immobilized by a cervical collar have limited neck mobility.

The formal steps of RSI are shown. There are 2 essential components: induction and paralysis. Induction refers to creating an unresponsive state by the administration of a sedative such as etomidate or propofol. Paralysis refers to causing muscular relaxation by the administration of a paralytic agent such as succinylcholine or vecuronium. RSI maximizes the rate of successful intubation, decreases the risk for aspiration, and offers better C-spine control. The risks of undertaking RSI should be well understood, including prolonged intubation time, adverse drug effects, and development of a crash airway where none previously existed. RSI is unnecessary and inappropriate in patients who are in cardiac arrest.

The modified jaw-thrust technique (shown) can be employed in patients in whom a cervical spine injury is suspected. When properly performed, it can be accomplished without extending the neck. This maneuver uses the mandible to displace the tongue anteriorly, minimizing the tongue's ability to obstruct the airway. While standing at the head of the patient's bed, place the heels of both hands on the temporal-parietal areas on each side of the patient's head. Grasp the angles of the mandible with your fingers, and without flexing or extending the neck, displace the jaw anteriorly.

Once the patient is preoxygenated, sedated, and paralyzed, placement of the ETT is performed by introducing the blade into the right side of the mouth sweeping the tongue to the left and lifting the tongue up into the floor of the pharynx. Once a view of the larynx is obtained via laryngoscopy, the ETT is introduced with the dominant hand through the right side of the mouth (shown). Directly observe the tip of the tube passing into the larynx, through and 1 cm past the vocal cords. The distal cuff is inflated and positive pressure ventilations are provided. The lungs are immediately auscultated bilaterally for equal breath sounds as end-tidal CO2 is measured. Note the depth of insertion of the ETT at the lip line and secure the tube in place

Once the ETT has passed through the vocal cords, the stylet is carefully removed and the distal balloon cuff inflated with a 5- to 10-cm3 syringe. A BVM is attached, and the patient is manually ventilated to assess breath sounds and lung compliance. Confirmation of placement and proof includes visualizing the tube passing through the vocal cords (shown); equal breath sounds should be auscultated bilaterally with an absence of breath sounds over the epigastric area in the adult (pediatric patients may have referred breath sounds). The cartilaginous tracheal rings are also shown here (yellow arrow)
A postintubation chest x-ray does not confirm tube placement, but will evaluate the depth of ETT insertion (yellow arrow) in relation to the carina (red arrow), left or more commonly right mainstem bronchus intubation, and complications such as pneumothorax. An orogastric tube is then often placed to decompress the stomach, and an arterial blood gas is obtained and evaluated

The LMA is used as a rescue airway device to ventilate patients when traditional endotracheal intubation is impossible. The LMA is a cuff device that provides sufficient seal to allow positive-pressure ventilation to be delivered. It is especially useful in cases in which the laryngoscopic view is limited by an inability to optimally position a patient's neck, as in cases of trauma. Although the LMA may make ventilation easier, it does not protect the airway the way in which a cuffed ETT does, and thus it is desirable to transition to a cuffed ETT as soon as feasible. Difficult or failed bag-mask ventilation and failed intubation are the most common reasons for using the LMA in the emergency setting

An LMA has a large bore tube with a connector at the proximal end that is connected to a BVM or ventilator. The elliptical cuff at the distal end is inflated after insertion to form a low-pressure seal around the entrance into the larynx. The LMA comes in a variety of pediatric and adult sizes, and successful insertion requires appropriate size selection. The LMA will usually have the size, the suggested weight, and required volume of air needed to properly inflate the cuff (shown) printed on the side. The LMA is usually a successful device for rescue ventilation in the "cannot-intubate/cannot-ventilate" situation. Advanced cardiac life support guidelines suggest that the LMA provides a more secure and reliable means of ventilation than BVM ventilation

In preparation for LMA insertion, inflate the cuff to ensure that it does not leak. Then deflate the cuff to form a smooth flat wedge shape (left image) that will pass easily around the back of the tongue and behind the epiglottis. Use a water-soluble lubricant to lubricate the back of the LMA. The best patient position for LMA insertion is the sniffing position, with the neck flexed and the head extended, unless the patient has a suspected or known neck injury. Insert the LMA with the posterior tip pressed against the hard palate just behind the upper incisors. Under direct visualization, use the index finger to slide the LMA along the hard palate and into the oropharynx (right image)

While inserting the LMA, extend the index finger and push the cuff along the soft palate and into the posterior pharynx (left image) while the other hand provides counterpressure on the back of the patient's head (right image). Push the LMA into the hypopharynx until you feel resistance. After the LMA is inserted, inflate the cuff just enough to achieve a good seal with the glottis, which may only require half of the maximum cuff volume. Never overinflate the LMA cuff. Finally, attach a bag and ventilate the patient using chest rise, breath sounds, and capnography to confirm adequate gas exchange. The LMA does not completely protect against aspiration and may actually cause vomiting if the patient is not fully sedated

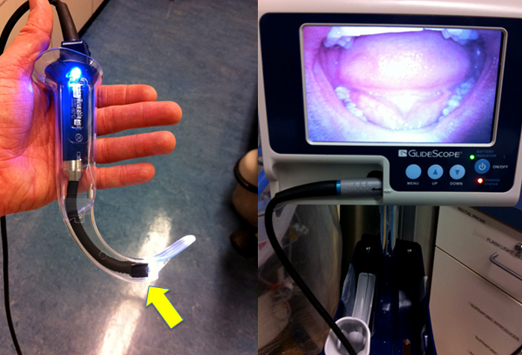
Video laryngoscopy affords more grade 1 and 2 views than direct laryngoscopy and improves glottic exposure in most patients with poor direct glottic visualization. The GlideScope video laryngoscope works primarily like a traditional laryngoscope with a 60° angulated Macintosh blade (left image). The video feed is projected onto an accompanying screen (right image). The digital video camera and light source are located at the point of angulation of the blade (arrow). The plastic blades are disposable and come in different sizes. Indications for GlideScope video laryngoscopy include morbid obesity, poor direct laryngoscopic view from trauma or anatomic variation, inability to view the vocal cords, small mouth opening (< 3 cm), limited neck extension, or suspected cervical spine injury

While looking at the mouth, insert the GlideScope into the midline of the oral cavity (left image). Then while looking at the monitor, elevate the tip of the blade to see the epiglottis and vocal cords (right image). Next, while looking at the mouth, insert the ETT and stylet into position near the tip of the GlideScope. The GlideScope has an antifogging heat lamp that heats up to 106° in 10 seconds enabling views in the presence of blood and secretions. Excessive blood and secretions should always be suctioned
While looking at the monitor, with the tip of the ETT at the vocal cords, gently pull back the stylet 1-2 cm and pass the tip to the ETT through the vocal cords intubating the trachea (shown). In clinical studies, GlideScope intubation was almost twice as successful and one third faster than conventional laryngoscopy
If oral intubation has failed and you are unable to oxygenate or ventilate using an airway adjunct, a cricothyrotomy can be employed to establish airway control with a tracheostomy tube. Other indications for a cricothyrotomy are massive oral, nasal, or pharyngeal hemorrhage; masseter muscle spasm; clenched teeth; structural deformities of the oropharynx; stenosis of the upper airway; laryngospasm; mass or tumor; airway obstruction; and oropharyngeal edema. Tracheostomy tubes come with an inflatable balloon and variable luminal diameters. The chosen tube should be three fourths the diameter of the trachea
When performing a cricothyrotomy, if you are right-handed, stand on the patient's left side and palpate the depression over the cricothyroid membrane with the nondominant hand. With the dominant hand, use a scalpel to make a single vertical 1.5-cm incision through the skin and subcutaneous tissue and then a horizontal incision through the cricothyroid membrane (red arrow).
With the scalpel blade still in place and a tracheal hook in the nondominant hand, using the inferior aspect of the scalpel blade as a guide, hook the cricoid cartilage with the tracheal hook. Then in a manner similar to the traction applied during oral laryngoscopy, use the hook with the nondominant hand to pull upward providing traction to dilate the membrane and stabilize the trachea (shown)

Next place a size 4 cuffed tracheostomy tube or size 6.0 cuffed ETT through the opening (shown). Often the most difficult part of this procedure is placing the tracheostomy tube into the small incision. An alternate approach is to pass a gum elastic bougie into the trachea first and then advance the ETT over the bougie. If using a tracheostomy tube, with trocar in place and outer cannula lubricated, insert the tip through the opening initially oriented in the transverse plane parallel with the Trousseau dilator. Rotate the dilator and tube together 90° inferiorly, and then advance the tube until the flange rests against the neck

Once the flange of the tracheostomy tube is flush against the neck, inflate the cuff and remove the trocar and the hook (shown). Proper placement of the tracheostomy tube is confirmed in the same manner as with ETT placement: assessment of end-tidal CO2 partial pressure, bilateral chest movement, and breath sounds. After confirming proper placement, suture the tracheostomy tube into place and obtain a postprocedure chest x-ray




































{kind=link}
{kind=link}
0 komentar :
Posting Komentar